Drowning is one of the most preventable tragedies in the world, yet it remains the leading cause of death for children aged one to four in the United States. A primary reason prevention efforts fall short is a widespread misunderstanding of how submersions actually unfold. Misleading, non-medical terms like “dry drowning” or “secondary drowning” only cloud public awareness.
This guide details the accurate types of drowning, the reality of silent submersions, and critical risk factors, along with actionable, lifesaving steps based on current safety research. It focuses entirely on factual, positive safety information to assist with family preparedness.
Drowning is clinically defined as respiratory impairment resulting from submersion or immersion in a liquid. In plain terms, defining what is drowning means looking at what happens when fluid blocks the nose and mouth long enough to completely halt normal breathing. This blockage quickly cuts off the body’s oxygen supply, triggering a state of hypoxia that can lead to irreversible brain damage, cardiac arrest, and death within a matter of minutes.
A critical point that often surprises the public is that drowning can be either fatal or nonfatal. While surviving a submersion event is entirely possible, surviving without long-term consequences is not guaranteed.
The global scale of this crisis is massive, with the World Health Organization estimating that approximately 236,000 drowning-related deaths occur each year making it the third leading cause of unintentional injury death worldwide. Drowning statistics consistently show a heavy burden beyond mortality, as roughly four nonfatal cases require formal medical evaluation for every single fatal drowning.
Because clear communication is vital when tracking these safety statistics, medical experts emphasize that terms such as “wet drowning”, “dry drowning”, “near-drowning“, and “secondary drowning” are no longer accepted medical terms.
Major health organizations, including the WHO, CDC, American Red Cross, and International Lifesaving Federation, have formally retired these labels in favor of standardized terminology. Although these confusing descriptions still frequently appear across parenting blogs and mainstream websites, they reflect outdated science and can dangerously delay critical, lifesaving care.

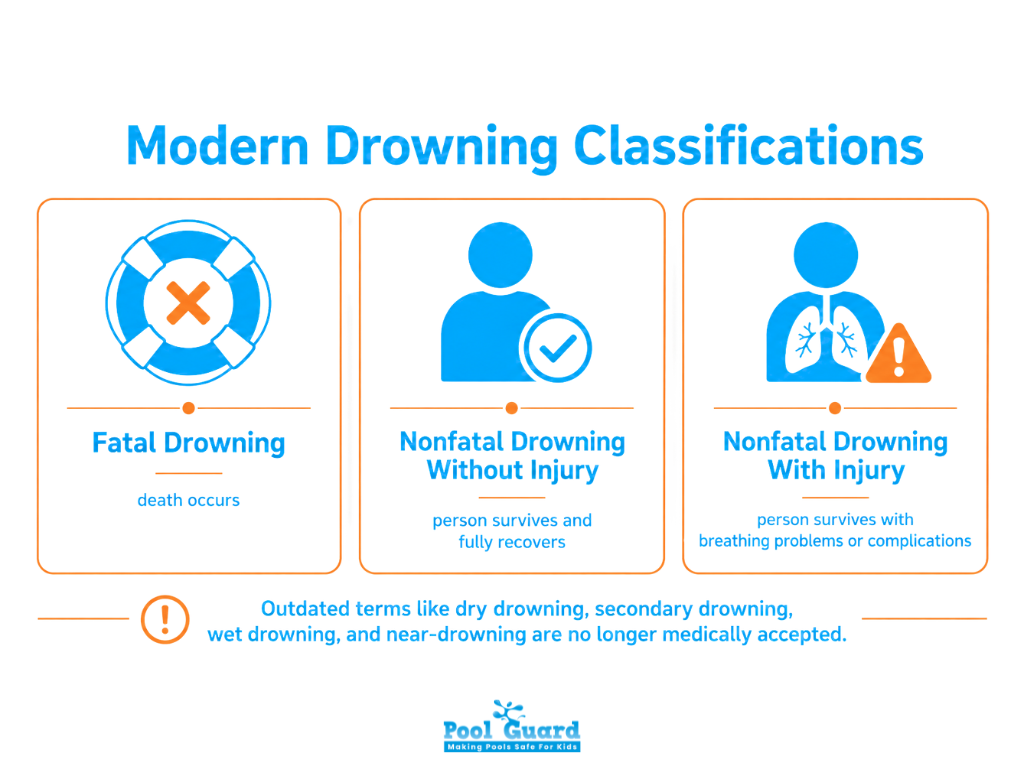
Modern clinical classification organizes drowning into three outcome-based categories. These standardized definitions are used by emergency physicians, public health researchers, and resuscitation guidelines worldwide to replace outdated and confusing terminology.
Fatal drowning results in death. This outcome occurs when the victim cannot be resuscitated at the scene or when subsequent medical interventions in an intensive care setting fail to reverse the damage caused by prolonged oxygen deprivation. It represents the ultimate tragedy that public safety campaigns, pool barriers, and lifeguard supervision work hardest to prevent.
Nonfatal drowning without injury occurs when a person is rescued, survives, and experiences no lasting respiratory problems or long-term health complications. Following a brief period of monitoring, a full recovery is made because the airway was cleared before significant hypoxia developed. This positive outcome is far more likely when bystanders respond quickly and initiate CPR immediately.
Nonfatal drowning with injury occurs when the person survives but experiences breathing problems or other pool injuries or complications afterward. Clinicians categorize severity across a clear spectrum. Mild cases involve uncontrollable coughing while fully conscious. Moderate cases feature visible breathing struggles and mental confusion. Severe cases are critical emergencies where the victim is unconscious and has stopped breathing.
Ultimately, long-term health outcomes depend entirely on two factors. These are the total submersion time and the speed of the initial rescue response.
Beyond outcome classification, drowning is also described by the behavioral circumstances of the event. These four types appear frequently in water safety education and are worth understanding.
Active drowning is the version most people picture – a person struggling visibly at the surface, arms pushing down on the water, body upright, unable to call for help. It typically occurs when someone recognizes they’re in danger and is physically fighting to stay above water. Despite the movement involved, active drowning is often much quieter than Hollywood depicts.
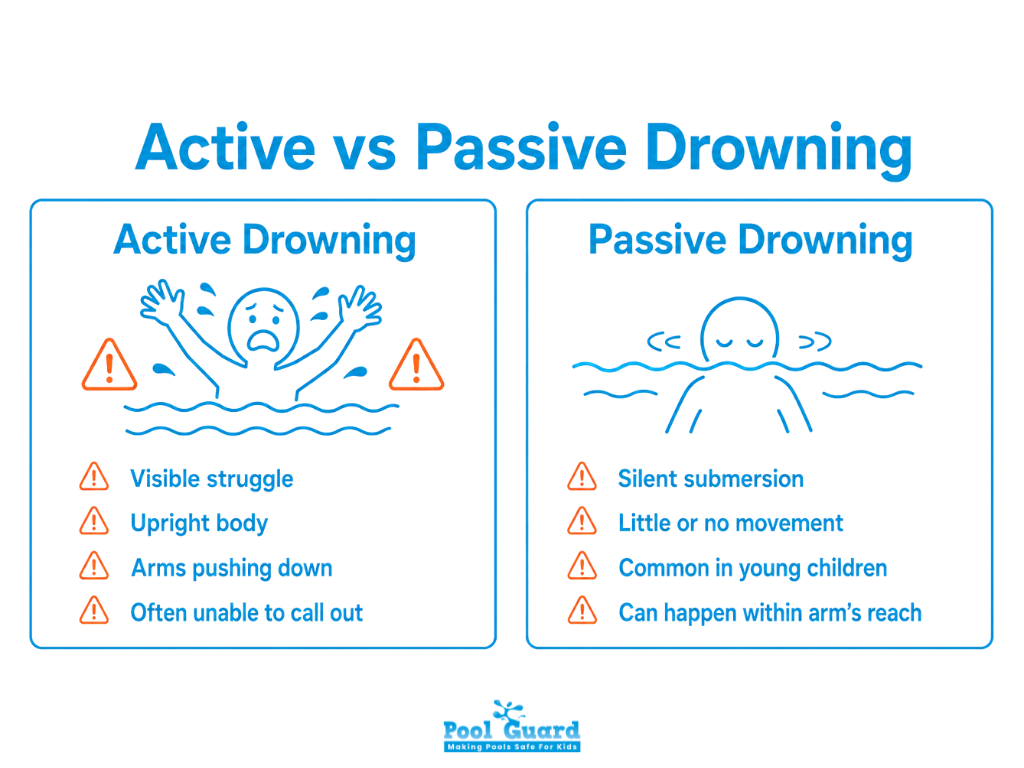
Passive drowning occurs when someone slips beneath the surface without struggle – no splashing, no calling out. It most commonly affects young children who lack the physical ability or awareness to fight back, and adults who lose consciousness due to a medical event, exhaustion, or intoxication. This is why visual supervision alone isn’t enough, as passive drowning can happen in complete silence within arm’s reach of an adult.
As outlined above, the submersion results in death, either at the scene or following failed resuscitation.
The person is rescued and survives. Survival without complications is possible, but any submersion event requiring rescue warrants medical evaluation. Importantly, mild or no symptoms following rescue don’t guarantee that nothing needs to be monitored.
It’s worth noting that classification systems vary across sources, and older frameworks may still use deprecated terms. When in doubt, rely on guidance from the CDC, WHO, or the American Heart Association.
Understanding how drowning progresses helps bystanders recognize warning signs faster. The process follows a predictable sequence, and every stage that passes without intervention reduces the odds of a full recovery.
The first response to losing control in water is panic. The body goes vertical, arms push against the water surface, and the person attempts to keep their airway clear. Swimming becomes impossible as exhaustion takes over. This stage typically lasts 30 to 60 seconds.
Once submerged, the victim holds their breath. How long varies, as water temperature, clothing, and physical condition all play a role. In warm water, breath-hold time may reach one minute; in cold water, it’s significantly shorter. As carbon dioxide builds in the bloodstream, the urge to breathe becomes overwhelming.
Water entering the airway rapidly lowers blood oxygen levels. The brain receives less and less oxygen. Most victims lose consciousness within two minutes of submersion. Once unconscious, the victim can no longer protect themselves.
Without oxygen, the heart follows the brain into failure. Most drowning victims enter cardiac arrest within five minutes of going underwater. Research shows that 88% of people who survived drowning were underwater for fewer than six minutes, which underscores how critical immediate response is.

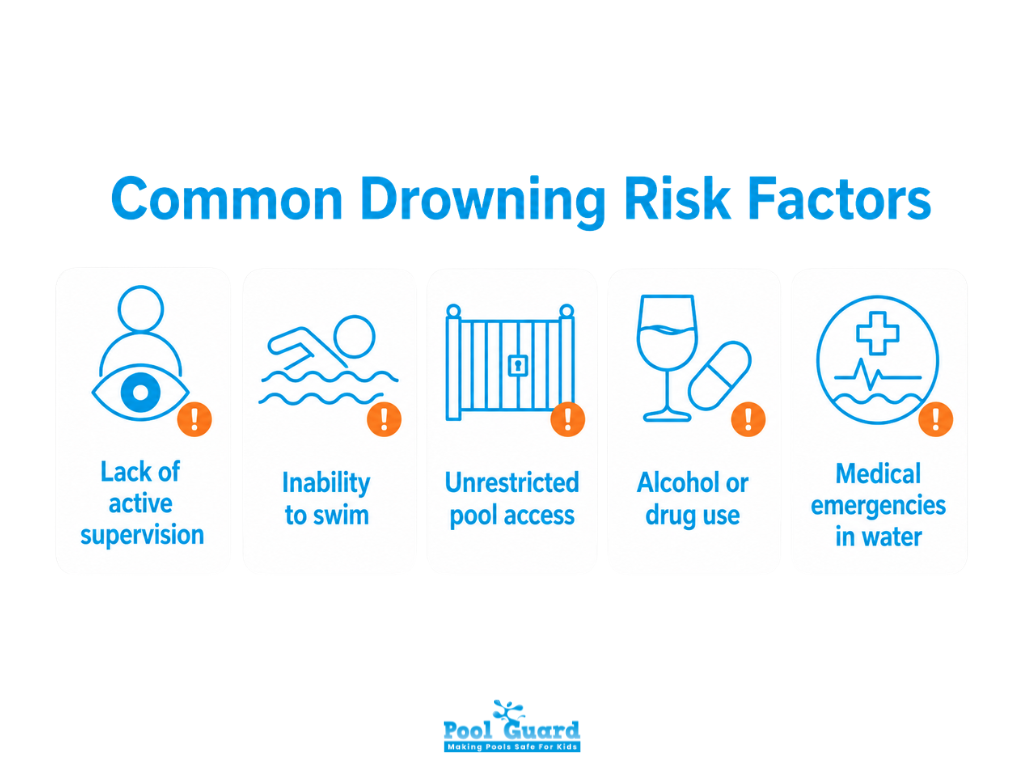
Drowning is not random. Specific, identifiable risk factors recur across the research, and most are controllable.
Most infant drowning deaths occur within five minutes of an adult looking away. Supervision gaps are the single most common factor in child drowning incidents. Passive supervision, glancing up from a phone, isn’t the same as active supervision.
Non-swimmers and weak swimmers face a significantly higher risk of drowning. A 2014 American Red Cross survey found that while 94% of parents expected their children to engage in water activities, only 39% reported their child could perform all five basic swimming skills. These findings indicate a significant gap between water exposure and proficiency in water safety among children aged 4-17. That gap is dangerous.
Racial disparities in drowning risk are also pronounced and well-documented. Black children and teenagers ages 5-19 drown at a rate 5.5 times higher than their white peers, a gap largely linked to historical inequities in access to swimming instruction.
Children frequently gain access to pools through unlatched gates or unfenced yards. Even children who have taken swimming lessons can drown if they enter a pool unsupervised. A four-sided pool fence with self-closing, self-latching gates is one of the most evidence-backed drowning prevention tools available.

Alcohol is associated with around 50% of adult drowning cases. It impairs judgment, coordination, and reaction time, and it accelerates hypothermia. Recreational drug use carries similar risks. The combination of open water and impaired decision-making is consistently fatal.

Heart attacks, cardiac arrhythmias, seizures, and hypoglycemia can all strike while someone is in the water, turning a routine swim into a drowning event. Adults over 65 and individuals with epilepsy, autism, or cardiovascular conditions face elevated risk. This is why swimming alone is dangerous even for experienced swimmers.
Yes, and this is one of the most important facts for any parent or caregiver to internalize.
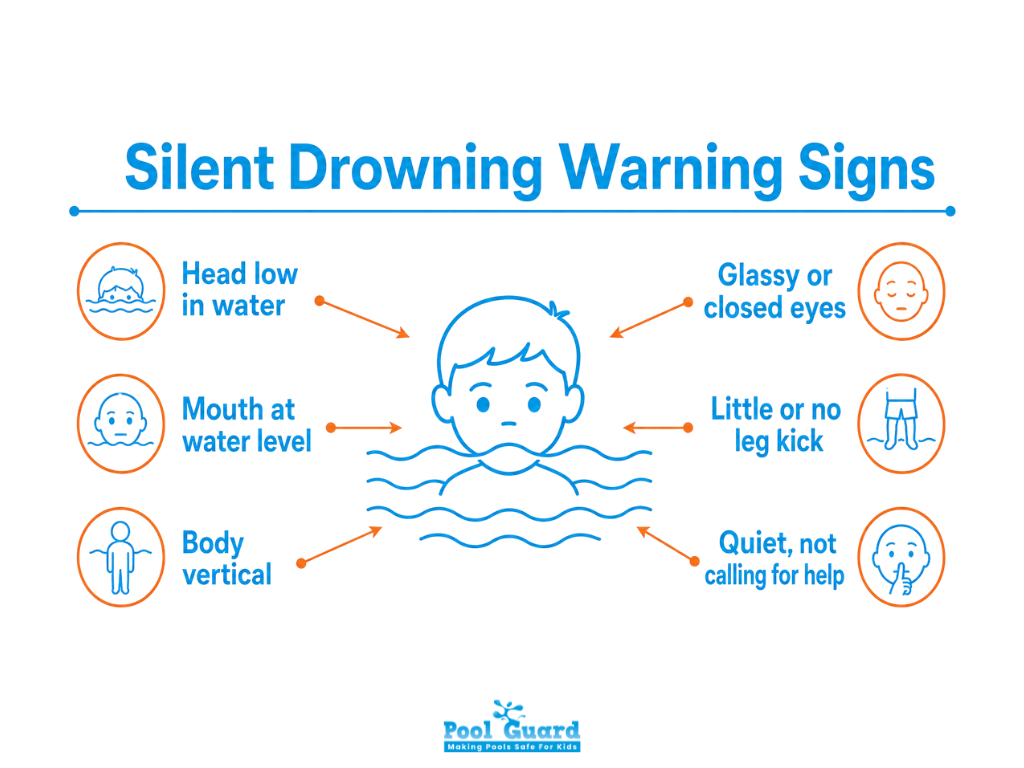
The dramatic movie scene of a person thrashing and screaming for help is the exception, not the rule. In reality, a drowning person cannot call out for help. When the body is fighting to breathe, the respiratory system takes priority – speech requires exhaling, which requires spare breath that a drowning person doesn’t have.
Warning signs are subtle: the body is vertical in the water rather than horizontal, the head is low with the mouth at water level, the eyes are glassy or closed, the hair covers the face, and there is little or no leg kick. A child who has gone quiet in the pool can be a more urgent warning sign than one who is splashing noisily.
Passive drowning, the type that claims young children most often, produces no visible struggle at all.
The encouraging fact is that over 90% of drowning incidents are preventable. These are the interventions with the strongest evidence.
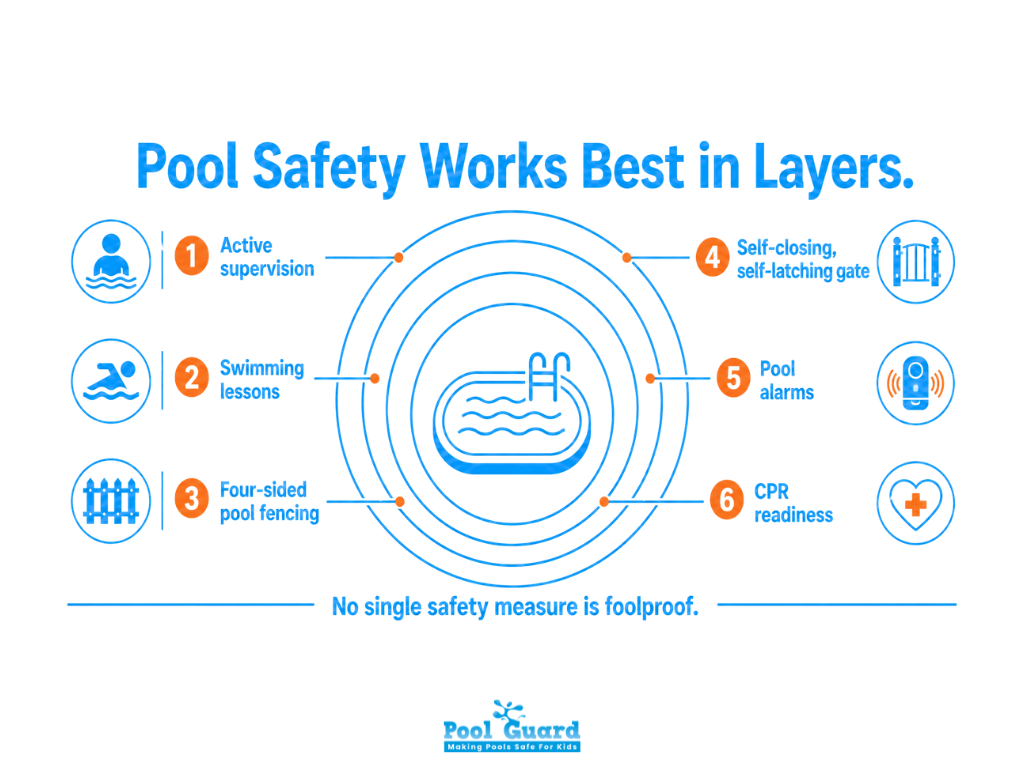
Designate a Water Watcher, one adult whose only job is to watch the water, with no phone, no conversation, no distractions. Rotate this responsibility every 15-20 minutes to maintain focus. No level of swimming ability makes a child exempt from this rule.

Formal swimming instruction significantly reduces the risk of drowning. Children as young as one can begin water familiarization. The goal isn’t just stroke technique; it’s water competency: the ability to enter the water, float, change position, and exit safely.

Four-sided isolation fencing completely encloses the pool and separates it from the house, reducing the risk of child drowning by up to 83% compared to three-sided fencing that uses the house as one wall. Pool safety gates must be self-closing and self-latching, with latches out of reach of small children.

No single safety measure is foolproof. Pool alarms, including surface wave sensors, subsurface motion detectors, and door/gate alarms, provide an additional alert layer for when other barriers fail. Wearable personal alarms for young children add yet another layer. The goal is redundancy – multiple barriers mean multiple chances to catch a dangerous situation before it becomes fatal.
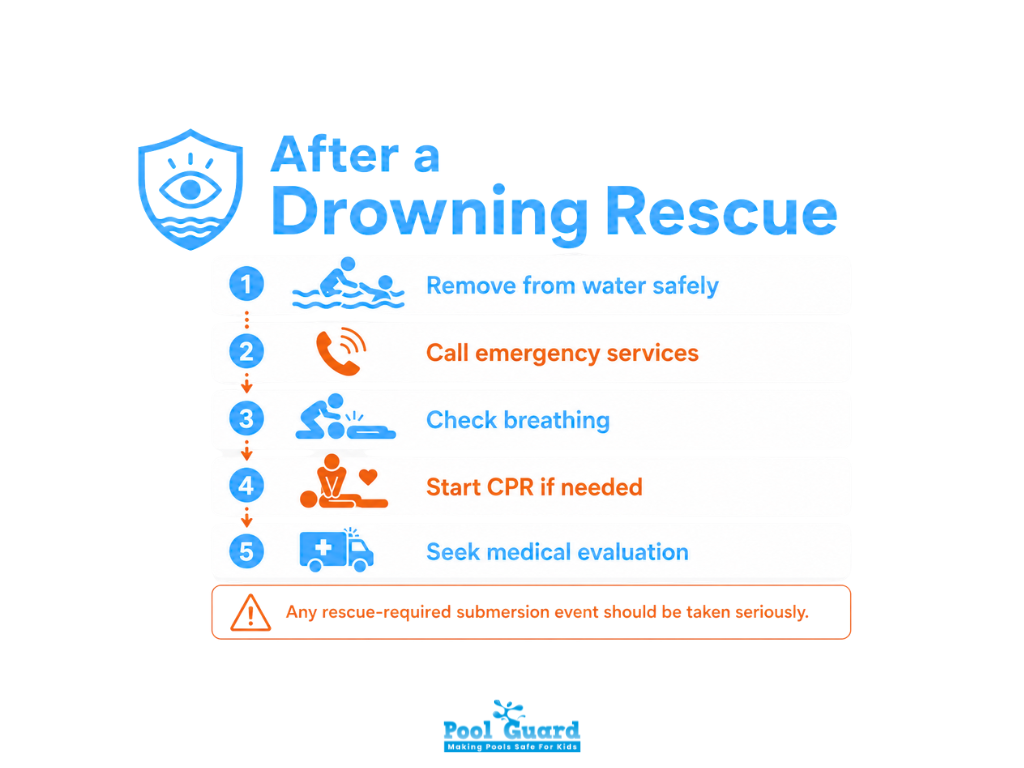
Bystander CPR is one of the most powerful predictors of drowning survival. Drowning CPR protocol calls for five initial rescue breaths before chest compressions, different from standard CPR, because the priority is restoring oxygen to a hypoxic victim. Every adult in a household with a pool should be trained and up to date.
Keep emergency numbers visible and know where the nearest automated external defibrillator (AED) is located. Note that AEDs are only effective in 2% to 14% of drowning cases. Because drowning-related cardiac arrest is caused by oxygen deprivation rather than a primary heart issue, delivering immediate rescue breaths takes priority over a shockable rhythm.

Drowning is fast, silent, and entirely preventable. True water safety means understanding modern medical facts: a quiet struggle rarely involves splashing or shouting, strong swimmers are never fully immune, and proper supervision demands active visual tracking rather than simple physical proximity.
Because a submersion injury unfolds in mere seconds, survival depends completely on the speed of the rescue response. Proper preparation bridges this critical gap. Learning about the actual types of drowning serves as the essential starting point for auditing your pool barriers, refreshing your household CPR training, and ensuring every adult knows exactly how to spot a silent emergency in the water.

Please fill out the form below with your information. Your local dealer will be notified about your inquiry.
Please fill out the form below with your information. Your local dealer will be notified about your inquiry.


